EXECUTIVE SUMMARY
The behavioral health finance problem is structural, not operational
Behavioral health organizations — inpatient psychiatric facilities, outpatient mental health clinic networks, substance use disorder treatment programs, group home operators, and integrated behavioral health providers — operate in one of the most financially complex segments of the healthcare industry. They bill across more payer types simultaneously than almost any other healthcare sector: Medicaid and Medicare for a large portion of their patient population, commercial insurance with mental health parity requirements, state-funded block grant programs with their own billing and reporting rules, and in some programs grant revenue from federal or foundation sources.
Each of those payer types has different billing requirements, different reimbursement rates for the same service, different prior authorization thresholds, and different timelines for adjudication and payment. Managing this complexity in a single accounting system that was designed for a simpler revenue structure is what generates the specific financial problems behavioral health CFOs deal with every month: unexplained variance between billed and collected, A/R aging that no one can explain, close cycles that produce unreliable consolidated financials, and audit findings that recur because the controls in place cannot keep pace with the operational complexity.
This whitepaper addresses the financial management infrastructure that behavioral health organizations need — and why NetSuite, configured specifically for behavioral health operations by Archer Insights, addresses each of these problems at the system level rather than requiring the finance team to work around them.
THE MULTI-PAYER PROBLEM
Why behavioral health billing is harder than general healthcare billing
Every healthcare organization deals with payer complexity to some degree. What makes behavioral health different is the combination of Medicaid as the dominant payer for a substantial portion of the patient population, mental health parity law enforcement that creates ongoing billing disputes with commercial insurers, and the presence of state-funded programs that operate outside the standard claims adjudication system entirely.
Medicaid: the dominant payer with the most variability
Medicaid is the largest single payer for behavioral health services in the United States. For most inpatient psychiatric programs, substance use disorder treatment facilities, and community mental health centers, Medicaid accounts for 40% to 70% of total revenue. That concentration creates a financial dependency on a payer whose reimbursement rates are set by state legislatures, whose managed care organizations adjudicate claims with widely varying policies, and whose prior authorization requirements change frequently.
- Medicaid managed care organizations (MCOs) in most states each have different clinical criteria for behavioral health authorization, different billing code requirements, and different timelines for authorization decisions — all for the same clinical services
- Medicaid fee-for-service rates in most states have not kept pace with cost inflation, creating a systematic below-cost-of-care reimbursement environment for providers who rely on them
- Medicaid billing edits and claim rejections occur at a higher rate than commercial billing, requiring dedicated A/R staff for Medicaid-specific denial categories that do not apply to commercial claims
Mental health parity: the billing problem no one has fully solved
The Mental Health Parity and Addiction Equity Act (MHPAEA) requires commercial insurers to cover mental health and substance use disorder services at parity with medical and surgical benefits. In practice, commercial payers continue to apply more restrictive prior authorization requirements, higher denial rates, and more aggressive utilization management to behavioral health services than to comparable medical services — creating both operational burden and, for providers willing to appeal, significant revenue recovery opportunity.
- Prior authorization denials for behavioral health services run at two to three times the rate of medical service denials at the same commercial payers — each one requiring a documented clinical appeal to recover
- Length-of-stay management for inpatient psychiatric services is more aggressive than for medical admissions, creating census management pressure that affects both clinical and financial planning
- Parity compliance tracking — maintaining the documentation required to pursue parity violation complaints when commercial payers apply more restrictive standards — requires systematic data capture that manual billing workflows cannot provide
State grant programs: revenue that does not fit standard billing
Many behavioral health organizations receive funding from state mental health authorities, federal block grants, or foundation grants that are not claims-based revenue. These funds come with specific reporting requirements, allowable cost restrictions, and performance-based payment triggers that must be tracked against program delivery rather than patient billing.
When this grant revenue lives in a separate spreadsheet or a secondary accounting system rather than within the ERP, the finance team manages two parallel financial realities: the claims-based revenue in the accounting system and the grant-funded revenue outside it. Consolidating them at close requires manual work that is prone to error and nearly impossible to audit reliably.
The multi-payer accounting problem in concrete terms:
A community mental health center billing the same service at $120 (Medicaid FFS), $185 (Medicaid MCO), $240 (commercial insurance), and $0 net (grant-funded, reported separately) needs a revenue recognition system that handles all four simultaneously, tracks the expected payment against each, and surfaces variance when the actual payment differs from expected. Most ERP systems handle one or two of these well. NetSuite, configured correctly, handles all four.
GROUP HOME AND RESIDENTIAL FINANCE
The specific financial complexity of group home and residential program operators
Group home and residential behavioral health operators face a financial management structure that combines elements of a healthcare provider, a property manager, and a social services contractor simultaneously. Revenue may come from a state contract per diem, Medicaid waiver per diem, commercial insurance, or some combination — with different rates for different levels of care within the same facility. Costs include clinical staff, direct support professional (DSP) labor, housing and facility costs, food and supplies, and program activities, all of which need to be tracked at the program or facility level to demonstrate cost-per-day compliance with contract requirements.
Revenue complexity
- State contract per diems that are negotiated annually and must be tracked against actual census and occupancy
- Medicaid Home and Community-Based Services (HCBS) waiver billing with specific service authorization requirements per individual and per period
- Tiered per diem rates based on acuity or level of care that must be tracked per resident rather than per facility
- Ancillary services billing (transportation, medication management, therapy) that may go through a different billing pathway than the residential per diem
- Grant-funded program components that must be tracked separately from Medicaid-funded and privately funded components for both accounting and reporting purposes
Cost tracking complexity
- DSP labor costs that must be allocated by facility and by funding source to demonstrate cost compliance with state and Medicaid waiver contracts
- Individual resident cost tracking for Medicaid-funded residents whose cost of care must be reconciled against the per diem paid
- Facility costs (rent, utilities, maintenance) that must be allocated across the resident population for cost reporting and contract compliance
- Vehicle and transportation costs that may be billable to Medicaid waiver funds, directly to the state, or covered under the residential per diem depending on the contract
- Medication costs tracked at the individual level for residents whose medications are covered under the residential contract
THE NETSUITE SOLUTION
How Archer configures NetSuite for behavioral health financial operations
NetSuite's core financial architecture — multi-entity, multi-currency, multi-book accounting with a configurable chart of accounts and rules-based revenue recognition — provides the foundation for behavioral health financial operations. What Archer Insights adds is the behavioral health-specific configuration that makes that foundation work for the specific financial management requirements of multi-payer, multi-program, multi-location behavioral health organizations.
ARCHER BEHAVIORAL HEALTH CONFIGURATION FRAMEWORK
| Configuration area | What Archer builds | Problem it solves |
|---|---|---|
| Multi-payer revenue tracking | Payer-specific revenue accounts with expected payment logic per payer type; automated comparison of expected versus received | Variance between billed and collected is surfaced by payer, not buried in aggregate A/R |
| Program and grant accounting | Separate program accounts with cost allocation rules; grant revenue tracked against allowable cost categories | Grant reporting produced from the ERP rather than from a separate spreadsheet; allowable cost compliance auditable |
| Medicaid MCO billing logic | Payer-specific billing rules and authorization tracking per Medicaid MCO | Prior authorization gaps caught before claims go out; MCO-specific denial categories managed proactively |
| Parity tracking framework | Commercial payer denial tracking by service category with parity comparison data | Documentation base for parity complaints; denial recovery prioritized by value and recoverability |
| Group home per diem accounting | Per-resident, per-facility revenue tracking with census-based accrual logic | Per diem revenue recognized correctly based on actual occupancy; census variance tracked in real time |
| Multi-entity consolidation | Separate entity books per program or facility with automated intercompany eliminations | Consolidated financials across the organization available without manual assembly |
| DSP labor allocation | Labor cost allocation by facility, funding source, and program | Cost reporting for state and Medicaid contracts produced from the ERP; DSP cost compliance auditable |
AUDIT AND COMPLIANCE
What behavioral health auditors actually look for — and how NetSuite provides it
Behavioral health organizations face audit exposure from multiple sources: external financial auditors, Medicaid audits from state agencies and their contractors, HRSA or SAMHSA audits for federally-funded programs, and in some states OMIG or equivalent audit activities targeting Medicaid billing compliance. Each type of audit has different documentation requirements, but they share a common thread: the auditor needs to verify that services billed were authorized, delivered, documented, and reimbursed at the correct rate.
Financial audit
External financial auditors for behavioral health organizations focus on revenue recognition (are grants and Medicaid revenue recognized correctly?), internal controls (is there documented approval authority for financial commitments?), and multi-entity consolidation (are intercompany transactions properly eliminated?). NetSuite configured by Archer provides a documented approval trail for every transaction, correct revenue recognition by program and payer, and automated intercompany eliminations — addressing the three most common behavioral health financial audit findings at the system level.
Medicaid audit
Medicaid audits focus on whether the services billed were authorized, whether the documentation supports the level of care billed, and whether the cost reporting for cost-based reimbursement programs accurately reflects actual costs. Archer's configuration connects authorization tracking to billing records and links cost allocation to the appropriate program and funding source — giving auditors direct access to the documentation they need without requiring manual preparation from the finance team.
Grant audit
Federal and foundation grant audits focus on whether grant funds were spent on allowable costs, whether the cost allocation methodology is documented and consistently applied, and whether the financial reporting to the grantor matches the accounting records. Archer's program accounting configuration tracks grant expenditures against allowable cost categories in real time, making grant audit preparation a reporting exercise rather than a reconstruction effort.
Parity compliance
Mental health parity compliance documentation requires data on authorization rates, denial rates, reimbursement rates, and utilization management criteria across both behavioral health and medical benefits at the same commercial payer. Building this documentation base requires systematic payer-level tracking of every claim, denial, and payment — which Archer's revenue cycle configuration provides as a standard output of normal operations.
MULTI-SITE CONSOLIDATION
Closing the books across a multi-site behavioral health organization
Behavioral health organizations with multiple programs, facilities, or entities face the same month-end consolidation challenge as any multi-location healthcare operator — but with additional complexity from grant accounting, program-level cost reporting, and the Medicaid and state contract reporting that may require separate financial statements at the program level even when the organization is consolidated for GAAP purposes.
The Archer multi-entity configuration for behavioral health organizations handles this by maintaining separate program and facility books within a single NetSuite environment, with automated consolidation across all programs and entities for external financial reporting and automated program-level reporting for contract and grant compliance. The close cycle produces both outputs simultaneously rather than requiring the finance team to produce one and then manually reconstruct the other.
What this means for a multi-site community behavioral health center:
A CMHC operating eight outpatient programs, two residential programs, and a crisis stabilization unit across five locations — each with different funding mixes, different cost reporting requirements, and different billing staff — can produce consolidated financial statements for the board, program-level financial statements for each state contract, and grant expenditure reports for each funder from a single close cycle in NetSuite. Without this architecture, producing all three requires three separate processes and three separate opportunities for the numbers to not reconcile.
THE MARKET MOMENT
Why behavioral health ERP is underserved — and what that means for Archer
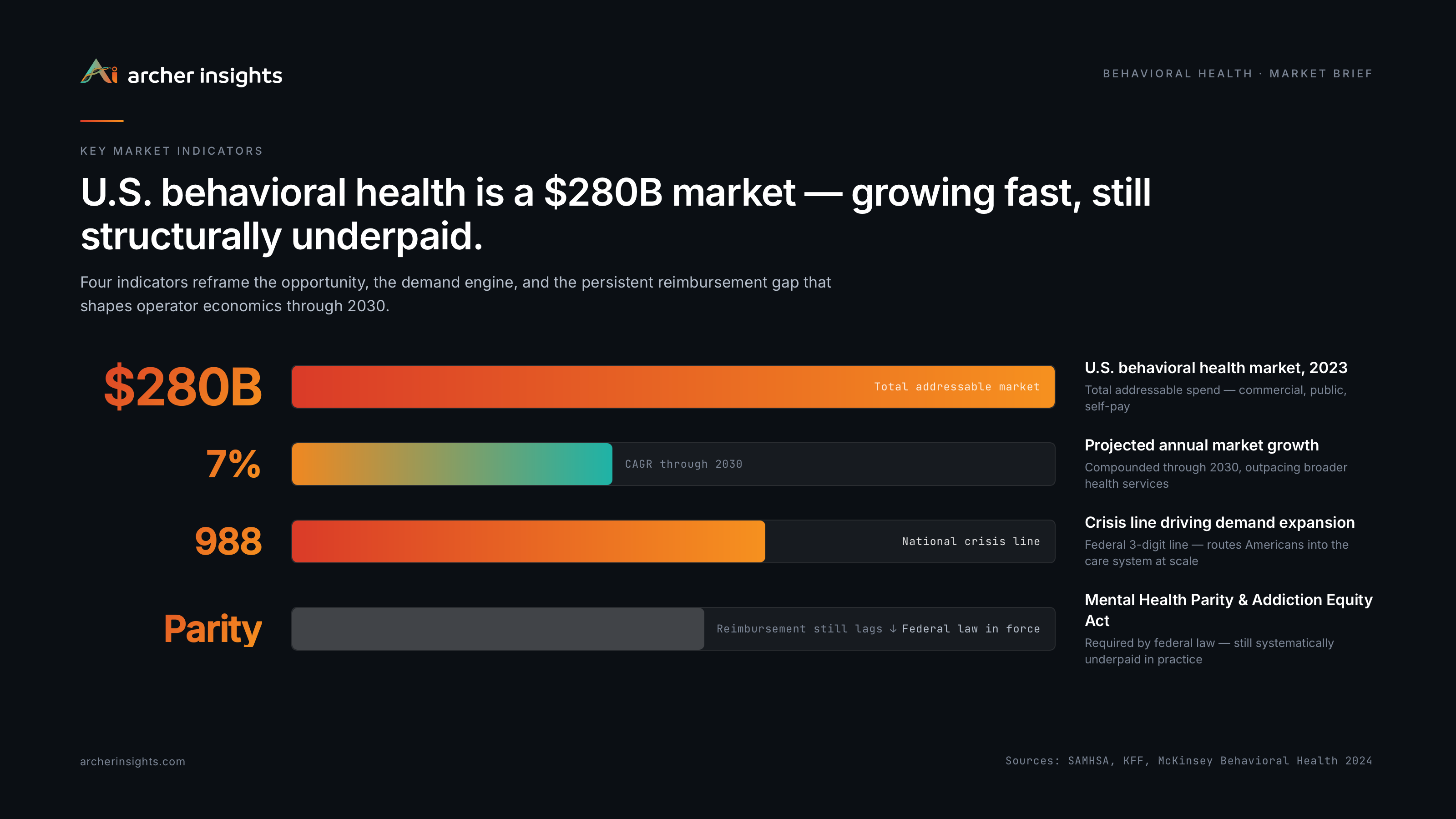
Behavioral health is one of the fastest-growing segments of the U.S. healthcare market, driven by the 988 Suicide and Crisis Lifeline expansion, mental health parity law enforcement, sustained investor interest in behavioral health platforms, and the expanding recognition of mental health and substance use disorder treatment as essential healthcare services rather than specialty add-ons. The market is expected to reach $500 billion by 2030.
Despite this scale and growth, behavioral health organizations are systematically underserved by ERP vendors. Most ERP partners that serve healthcare focus on acute care, physician groups, or health systems — markets with larger average deal sizes and more standardized financial structures. The multi-payer complexity, the grant accounting requirements, the DSP labor dynamics, and the program-level reporting requirements of behavioral health organizations are rarely addressed in pre-built ERP configurations.
Archer Insights built expertise in behavioral health financial operations through engagements with mental health center networks, substance use disorder programs, and group home operators. The configurations described in this whitepaper are not theoretical — they are operational in behavioral health organizations that chose to build the right financial infrastructure rather than continuing to work around the limitations of systems that were not designed for their environment.
Archer Insights is a five-time consecutive NetSuite Alliance Partner Spotlight Award winner (2022 through 2026), recognized specifically for its work in the Life Sciences and Healthcare sector. Archer's healthcare practice serves mental health organizations, behavioral health networks, residential programs, and specialty providers.
Call to Action
If your behavioral health organization is managing Medicaid billing, grant accounting, and program-level reporting across disconnected systems, Archer can show you what a unified, audit-ready financial infrastructure looks like.
archerinsights.com | Schedule a conversation with our healthcare team